As part of our on-going efforts to prototype and test new signage/way finding concepts for the hospital, the Marino Ward on level 14 recently had a set of prototypes installed. The Lab worked with staff and the service improvement manager who have been concentrating their efforts on initiatives to reduced the number of falls around the toilets and showers. The signage has been well received and similar to AED feedback, there is scope to develop backlighting for the designs.
Check out this super interesting read about the influence of good design on a patient recovery...
PLAINSBORO, N.J. — Can good design help heal the sick?
The University Medical Center of Princeton realized several years ago that it had outgrown its old home and needed a new one. So the management decided to design a mock patient room.
Medical staff members and patients were surveyed. Nurses and doctors spent months moving Post-it notes around a model room set up in the old hospital. It was for just one patient, with a big foldout sofa for guests, a view outdoors, a novel drug dispensary and a bathroom positioned just so....
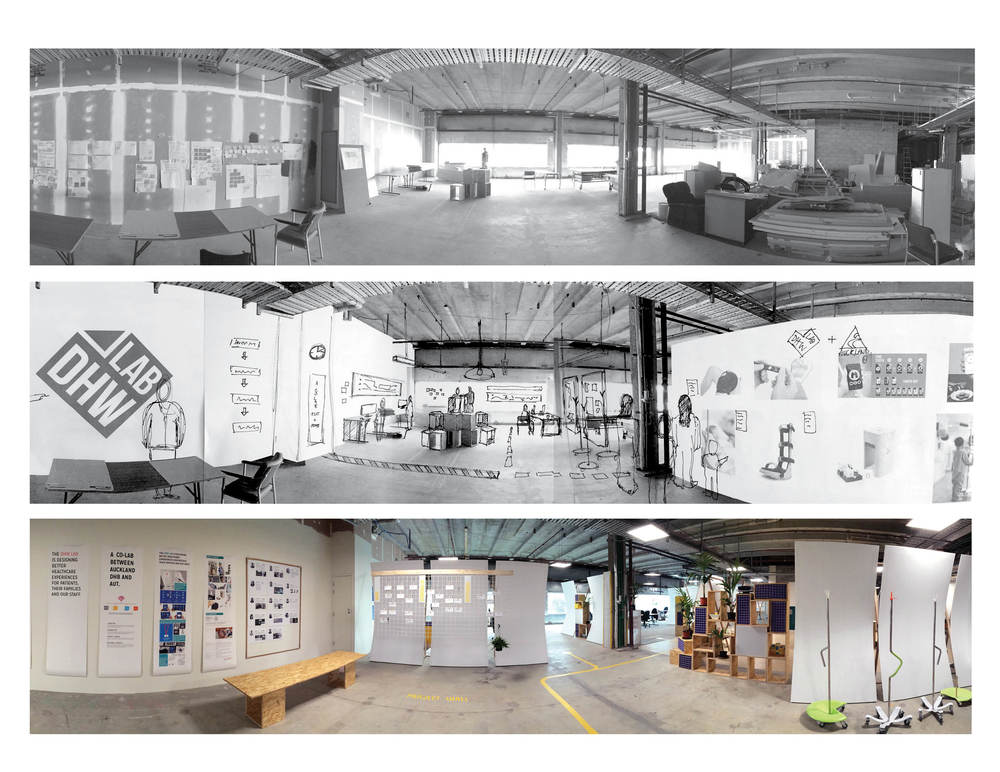
Its been a busy past month or so, designing and building a semi permanent fit out for our space at the Grafton Hospital. Occupying a physical space at the hospital has provides an environment for designers and hospital staff to meet and discuss opportunities on site, in order to develop trust between the two organisations.
The space will develop and change with its users.
Check out this interesting article where Fast Company talk to Joel Dudley about the powerful opportunities for creativity and design thinking to positively impact the health care industry.
Joel Dudley, one of Fast Company’s Most Creative People of 2014, is director of biomedical informatics for Icahn School of Medicine at Mount Sinai Medical Center in New York City and co-author of the book, Exploring Personal Genomics. His research focuses at the nexus of biology, medicine and big data to advance “precision medicine”--the tailoring of health care to each individual’s unique molecular composition to better treat and prevent disease.
What does it mean to you to be creative in health care?
Creativity in health care versus other fields is not in its essence different. It’s just creativity. One way to define that is looking at things in new ways. In some of my work, it’s been re-looking at disease and re-imagining what it means to have a disease. We have a system now where disease is really broken up into artificial buckets. Disease is more likely a continuum, and the way to really reimagine those labels is through data.
Another aspect of creativity is bringing in perspectives from other areas and applying it in medicine. One example of that in my work is looking at the algorithms that Amazon might use to match products to shoppers, or that Google might use to match ads to people on a web browser--using that same approach of pattern matching--applying it in medicine to find new uses for existing drugs. We found that approach was indeed, in some ways, much more powerful than the very limited [drug] target-based approach or expert-based approach.
How can more creativity improve health care?
Creativity can help break down the artificial barriers that we have in medicine. We see medical specialties as being very different and very disconnected from each other--and they are largely driven by diseases. This leads to the idea that different parts of the body and different diseases are all disconnected. But we know that it’s all connected. It creates these very artificial barriers that need to be broken down.
What can better data or big data teach us about health that we didn’t know before?
We’re at an exciting time. With various technologies, whether they are imaging or genomic technologies, we can measure way more than we now know about the field. Although that’s actually a pretty new idea in medicine and biology, it’s actually a pretty old idea in physics and astronomy. People in those fields have already gone through this period where their technical capabilities were able to measure way more than they understood about the physical world. Medicine and biology has been pretty far behind where we haven't been in that position until now.
This brings about a couple of new things. There’s actually a new idea of humility in medicine and biology. We’ve never had to deal with the humility that we can actually gather more data than we understand--far more than we understand. So that’s a new thing. Because of that we need to be able to relook at all of the things that we thought we knew really well. We have these ideas about how biology works but we have to be willing to look at those again and potentially throw them away.
It’s almost as if you had six pixels across the screen and you watched all of Harry Potter. You could only see it through six pixels. You could infer some information, you could see things moving, and maybe detect some patterns. But now we have the full screen HD view of biology, and that means you need to watch the movie again. You need to take a second look at it. And your interpretation is going to be very different that way.
What’s your personal vision for the future of health care?
One aspect is that we will develop a learning health care system that is personalized, predictive, and adaptive. Right now we have these fleeting snapshots of an individual's life and they are not connected to each other. A new patient comes into the front door of the hospital, and aside from the knowledge that’s in the doctor’s head, we don’t learn from the historical data. I believe we will have a learning health care system that will constantly be adapting to the context of populations, of the location of individuals, and learning continuously from the data.
That will be enabled by the existing data that we have, but also new types of data that will come into the system. A lot of the way that we collect health information that may now be the exclusive domain of the hospital is going to move to the consumer--things like regular blood tests and health monitoring though devices. Places like Walgreens are going to be offering a lot more services than they do today. We’ll be able to collect this information in a more friendly way, but also in a more real-time way. We won’t just be trying to figure out your health based on the 1 day out of the 365 days a year that we see you in the hospital.
In the future, I have some hope that disease labels will completely go away. We won’t think about people as if they have a disease or not. Your health could really going to be described based on something like GPS coordinates. Based on all of the information we have about you, we know that you’re somewhere in the health and wellness universe compared to the rest of the world. So it’s not like you're in a bucket--you have GPS coordinates for your place in the health universe. Then what we can do is say this is where you are now. This is what people who have been in that same position this is what they did and this is what happened to them. We are starting to at least try to work towards this with some projects that we have here.
What’s a major impediment or challenge that you often come across and how do you tackle it?
One of the biggest impediments is dogmatic or reductionist thinking in medicine and biology. People are always wanting to zero in one small aspect of human physiology to either understand or treat disease. But humans are complex adaptive systems with billions upon billions of things interacting inside of us at multiple levels. And so this sort of reductionist thinking is a problem, and it’s not really compatible with the data-driven way things are going.
A related challenge is that human brains don’t really like to think quantitatively or probabilistically. Human brains are pattern-matching machines and storytelling machines. It’s hard for us to listen to the data or to understand things that are coming out data--for example, understanding our disease risk based on probabilistic information or what algorithms are telling us.
I don’t think we’re going to change human brains. Evolution is not that fast. The challenge is: How do you bridge this new world of medicine being very quantitative and data-driven with the fact that human brains don’t like to operate in that mode?
We’ve taken some early steps towards that. I was part of a group that published the first clinical interpretation of a human genome. One of the first challenges that arose from that is, wow, we’ve now assessed this individual for their risk for hundreds of different diseases. How do you present all of this information to clinicians? My part in that was to come up with a visualization that could fit on one page and would convey all of that. It actually leveraged some of the things that the human brain likes to use--patterns, colors, shapes--to transmit information.
What skill or mindset could the health care world use more of?
Two things. The health field needs more quantitative thinkers and it needs more design thinkers. Almost more stress on the latter. Health care needs a lot of people engaging in design thinking. We need people thinking about problems, thinking about potential technology and medial solutions, and how those things turn into better products for health care--people who are looking at it holistically like that, but with a mind toward better design.
The Auckland DHB has recently been working on a research project, to understand peoples' experience of the public spaces at the Grafton campus. The Lab has been involved in this project by developing the researching methods used to interview people, and in packaging up/documenting the project.
'We want to discover what our staff, patients, families and visitor’s current experience are of our public spaces within Auckland City Hospital. We have defined our public spaces to include the main entrances on levels 1, 4 and 5 and the retail space and eating areas on level 5.
We can only get this right if the people who use these places help us design a better place together.
How to get involved
To get this underway we are kicking-off with a Discovery Week 7- 13June. During that week there will be lots of opportunities for staff, our patients their families and other visitors to tell us: how you currently use the spaces; what you think about the shops and services on offer; how the entrances and exits work, and about the places to eat.
Have your say by completing our online survey or go along to the interactive workshop for staff on Thursday 12 June 10am to midday. To book a place emailfirstimpressions@adhb.govt.nz with your name, position and contact number.'
Honours student Lauren Hyland recently undertook a role-play exercise to help her gain empathy for elderly patients in public healthcare. Much more than a simple exercise in acting, Lauren fully transformed her visual appearance and identity, with the help of make-up artists at BodyFX, into that of an ill-looking, frail elderly woman. Following her radical transformation, Lauren immersed herself in the context of public healthcare at Auckland City's Public Hospital at Grafton, providing her an interactive environment to act out the experience of her users. Lauren reflects on the exercise and her experience below:
This practice-based research project explores the complexity of human needs and social values to assess how physical privacy for vulnerable patients can be improved through a product design intervention. Through the application of Human-Centred and Universal Design frameworks, this project focuses on addressing the needs and values of our ageing population through empathic design.
My key insights were gained through the use of ‘Role-Play’ as an explorative, empathy gaining method. With the help of BodyFX - the make-up & prosthetics specialists - I was able to fully embody what it is like to be an elderly patient by experiencing a day walking in their shoes. I allowed myself to be immersed into the moment - feeling vulnerable, overwhelmed and at times invisible or ignored.
This has proven to become my most valuable research method to date, providing myself with the experience and empathic understanding for how I might implement a design intervention to better meet the needs of the elderly and ultimately preserve their dignity in care.
These insights reflect a key milestone in my project’s purpose and direction going forward. With these considerations in mind, I have developed a new problem statement: how might we provide protection and privacy for elderly patients whilst supporting their visibility in care?